
Treatment planning the Posterior Maxilla II: Prosthetic design and patient-related variables
By Gary Steen, DDS. DICOI, AFAAID, FAGD, MeCSD, MBA
Thoughtful treatment planning should be microscopic and should hold foremost the well-being of actual bony trabeculae adjacent to our implants. How goes the health of these delicate structures goes the health of our implants? Failure rates in the maxilla have been reported to be as high as 30% because of the difference in trabecular, and to a degree cortical, structure between the two jaws (1) (2). Mandibular rules don’t always apply when we are short-changed BIC (bone-implant contact) in the sparsely-trabeculated rear maxilla. More than anywhere else, if we can distill all our maxillary treatment planning choices down to a single rule, it should be “protect those fragile trabeculae.”
The patient’s past and current health, medications, age, sex, diet, habits, and attitude are parts of a broad discussion that may be best deferred. It’s enough to say that any aspect of these that affect our all-important BIC becomes critical, and can easily change, and even abort, our treatment. To narrow the focus on prosthetic design, we’ll zoom in on how our choices affect just the bone/implant complex.
The patient deals the cards, and we must play them. Implant-related factors such as favorable surface treatment, adequate size in both width and length, and an appropriate thread pattern can improve BIC, as we have seen. Patient-related factors such as bone quality and volume, genetics, occlusion, and the way in which he or she applies forces to the teeth will affect our outcomes, as will the design of the prosthesis that receives and transfers these forces to bone.
 Protecting bone with prosthetic strategies, in view of limited BIC in the patient, is the focus of this discussion.
Protecting bone with prosthetic strategies, in view of limited BIC in the patient, is the focus of this discussion.Patient bone density and prosthesis design. Wide spacing between trabeculae in type 4 maxillary bone gives it the lowest BIC in the jaws. The voluminous intertrabecular matrix offers nothing for implant support. A thicker cortical plate adds to overall BIC in the mandible, but the posterior maxilla presents some of the thinnest cortex in the mouth and thus the least protection for the all-important trabeculae (4). Fig 1.
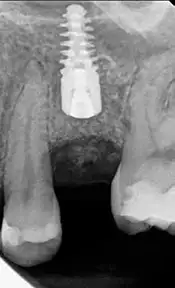
When bone structure provides only a low BIC, implant length becomes significant for initial stability and for adding back lost BIC (5) (2). Using this length to achieve bicortical stabilization between the crestal cortex and the sinus floor is a design strategy that offers significant protection to trabeculae between these denser layers. Jeong et. al. found a 20% reduction in trabecular stress as measured at the apical part of the implant when both plates were engaged (1). (Fig 2).
 Patient genetics and prosthesis design. Bone cells are sensitive to the topographical features of our implants, as we have seen, and will upregulate the expression of bone-forming genes in their presence (6). It’s important to remember that this upregulation may facilitate early stabilization and more rapid repair in remodeling, but the bone that results is still what had been programmed by that patient in that location.
Patient genetics and prosthesis design. Bone cells are sensitive to the topographical features of our implants, as we have seen, and will upregulate the expression of bone-forming genes in their presence (6). It’s important to remember that this upregulation may facilitate early stabilization and more rapid repair in remodeling, but the bone that results is still what had been programmed by that patient in that location.Densification of the osteotomy isn’t a shortcut or a rationale for using an undersized implant or fewer implants by assuming that the density increase will persist. The purpose of densification is short-term density increase for initial stability (7). The long-term nature of that bone remains constant and its underlying genotype will dominate. As remodeling progresses, that patient’s bone and original trabecular structure will have to support the materials that we introduce, and the forces that the patient introduces, forever.
Age also brings a slowdown in the genetic expression of bone forming factors. Actual bone mineral density decreases with time, as does cortical thickness and overall bone volume (8). Marginal design that works in a younger patient may not be appropriate in that same patient years later as the actual BIC for a given implant decreases. (Newton also points out that muscle mass and cross-section also decrease, which may offset some of the hard tissue changes with age.)
A good prosthetic design will assume that genetic determinants create a future of decreasing trabecular structure for implant support.
Patient occlusion and prosthesis design
Occlusal loads in the molar areas have been measured at an average of 723 N, with men as high as 847 N and women lower at 597 N (9). Bruxers have been measured in sleep with higher forces than they can generate when awake. Prosthetic design in the maxilla must address these forces in the face of the poorest supporting bone in the mouth.Stress on individual implants or teeth is affected by the completeness of the arch in which it sits. Relative load is increased in the absence of occluding neighboring teeth or implants, by the absence of contralateral occlusion, by absent anterior occlusion, and by teeth or implants in the opposing dentition. Good prosthetic design must ensure that axial forces applied by a given patient stay relatively constant and be shared between all available occlusal contacts, especially teeth. Non-axial forces are tolerated by teeth but must be avoided on implants. Full arch prostheses are best adjusted to a balanced occlusion and individual prostheses should allow adjacent teeth to absorb non-axial forces.
One prosthetic strategy for individual restorations uses the first molars for the most distal occlusal contact and treats the replacement of second molars as unnecessary (if even possible in the mandible). This can work well in small-muscled and older patients (10), but it may not be a universal prescription. The upper first molar is part of a working pair and its bone makes it easily the weak sister if it is to be replaced. If anatomy precludes creating a second molar pair, the maxillary first molar implant should ideally be positioned in both cortices (alveolar and sinus floor) and be as wide as possible. Misch suggests a 5 x 12 mm minimum dimension in this area. He also suggests that a pair of narrower implants may be superior to a single wide one (3). A single shim stock relief between the occlusal surface and its opposing surface helps minimize stress on the implant itself and ensures load-sharing with adjacent periodontal ligaments.
Patient forces and prosthesis design
Thoughtful distribution of chewing forces is a good design. A broad statement that may serve as a rule for force distribution in the mouth would be that good structural planning transfers forces to periodontal ligaments where possible, to the broadest area of bone around implants where possible, and to mucosa if all else fails.a) Periodontal ligament. Teeth have several things up on implants when they are subject to chewing and bruxing forces. The periodontal ligament (PDL) holds a shock-absorbing space around the root of approximately .25 mm in width that allows tooth movement within the bony housing. The lamina dura is a denser, cortex-like interface between the root and the trabeculae of the alveolus. The PDL provides tension forces to the lamina dura when the tooth moves and is stimulatory. Compressive forces are minimal except in trauma and in orthodontic movement. For the most part, the trabecular bone is minimally aware of applied forces.
So, the pathway of an applied force from the occlusal surface of a tooth to the surrounding trabeculae is via the flexible dentin of multiple roots to the fibrous PDL to the denser lamina dura and finally to the trabeculae. That’s a formidable line of defense for that bone. By contrast, a force applied to the occlusal surface of an implant is delivered through cold, hard titanium straight to the trabeculae. Good prosthetic design must keep the welfare of these little structures uppermost. If there are occluding teeth in either arch, transferring chewing forces to them allows the implant-supporting bone to share its defenses.
b) Bone area. Because stress is a function of both force and surface area (S=f/a), the resultant strain at the interface of trabecular bone and implant can be mitigated by either decreasing forces or increasing surface area. Macro forces are patient dependent and the implant dentist can generally do little to affect muscle size, muscle activity, jaw behavior, and diet. Initiating forces, thus, are a fixed variable, for the most part.
The received force, on the bone at each implant, can be modulated by utilizing cortical densities with bicortical placement and with wide-diameter implants, as we have seen. Maximizing the amount of available trabecular bone with ridge and sinus grafting will permit longer implants, which adds to BIC and thus distributes forces.
Splinting properly-sized implants is another strategy for distributing forces. The individual BICs of splinted implants are effectively summed in an axial direction. In non-axial directions, the splint’s bracing effect is meaningful. It’s instructive at this point to consider the total root surface area that we are replacing with cylindrical objects. Replacing the function of, say, 22 roots in the maxilla (4 molars) with 4 cylinders (often shorter than the original roots) supporting a horseshoe prosthesis, needs careful consideration. The bone is the same but diminished. That it can be successful even with 6 or 8 splinted implants is a testament to the effectiveness of splinting.
c) Mucosal support.
 For many reasons, it happens that adequate BIC to support a full prosthesis can’t be achieved without undue invasiveness, risk, or cost. Flange-related considerations of lip support and smile line are luxuries limited to implant-supported cases with realistic bone support for implants. Those considerations are moot if the patient’s bone gives a BIC that will only allow for an implant-retained prosthesis that is tissue-borne. The trabeculae holding these implants will, and must, lead a passive existence, free of compressive forces, if they are to endure. Occasional lifting forces when the prosthesis is removed are better tolerated. (Fig 3.)
For many reasons, it happens that adequate BIC to support a full prosthesis can’t be achieved without undue invasiveness, risk, or cost. Flange-related considerations of lip support and smile line are luxuries limited to implant-supported cases with realistic bone support for implants. Those considerations are moot if the patient’s bone gives a BIC that will only allow for an implant-retained prosthesis that is tissue-borne. The trabeculae holding these implants will, and must, lead a passive existence, free of compressive forces, if they are to endure. Occasional lifting forces when the prosthesis is removed are better tolerated. (Fig 3.)The posterior maxilla follows the fewest rules and requires the most consideration of any area of the mouth. As part of the larger skull, it was never stressed in evolution the way the isolated mandible was, and consequently never had to develop a denser structure. Our introduction of cylinders, with much less surface area than a triple rooted molar, and asking them to do the same job, is something new for this type of bone. We can succeed if we’re smart.
References
1. Jeong, et al. Bicortical Stabilized Implant Load transfer. Int J Oral Maxillofac Implants. 2003, Vol. 18, pp. 59-65.
2. Diaz-Sanchez, et. al. Improvement in the Initial Implant Stability Quotient Through Use of a Modified Surgical Technique. J Oral Implantology. June 2017, Vol. 43, 3, pp. 186-193.
3. Misch, Carl. Treatment Planning for the Edentulous Posterior Maxilla. Contemporary Implant Dentistry, 3rd ed. St. Louis: Mosby, 2008, p. 390.
4. Density of Bone: Effect on Surgical Approach and Healing. Contemporary Implant Dentistry. St. Louis: Mosby, 2008, pp. 645-67.
5. Sim, Lang. Factors influencing resonance frequency analysis assessed by Osstell mentor during implant tissue integration: I. Instrument positioning, bone structure, implant length. Clin Oral Implants Res. 21, Jun 2010, Vol. 6, pp. 598-604.
6. Stanford, CM. Surface Modifications of Dental Implants. Australian Dent J. 2008, Vol. 53, (1 Suppl), pp. 26-33.
7. Bradley Lahens, et. al. Biomechanical and histological basis of osseodensification drilling for endosteal implant placement in low density bone. An experimental study in sheep. J Mechanical Behavior of Biomed Mat. 2016, Vol. 63, pp. 56-65.
8. Huayue Chen, et al. Age-Related Changes in Trabecular and Cortical Bone Microstructure. Int J Endocrinology. 2013, Vol. 2013.
9. Costa Martins de Sa, et al. Fracture Strength of Standard and Small Diameter Prosthetic Abutments for Full-Arch Implant-Supported Restorations. J Oral Implantology. 2017, Vol. 43, 3, pp. 175-9.
10. JP Newton, et. al. Changes in human jaw muscles with age and dental state. Gerodontology. Jul 1993, Vol. 10, 1, pp. 16-22.